
Recent Updates in Venetoclax Combination Therapies in Pediatric Hematological Malignancies

 and
and
Abstract
:1. Introduction
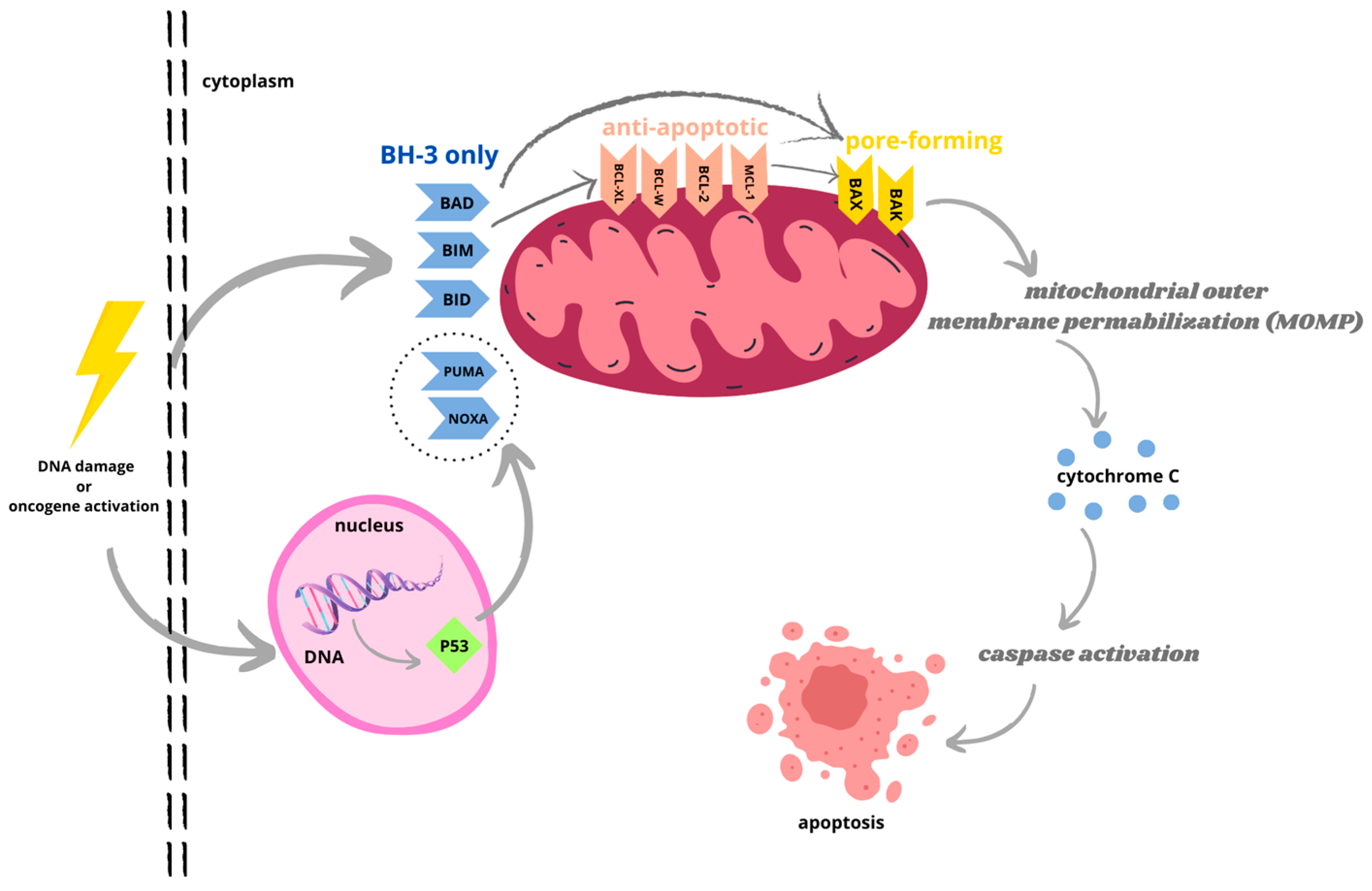
1.1. Apoptosis
1.2. B-Cell Lymphoma 2 (Bcl-2) Protein Family
- Antiapoptotic, e.g., BCL-2, BCL-XL, BCL-W, and MCL-1;
- BH3-only (proapoptotic), e.g., BIM, BID, PUMA, NOXA, BIK, and BAD;
- Pore-forming or ‘executioner’ (proapoptotic), e.g., BAX, BAK, and BOK.
1.3. Bcl-2 Inhibitors
1.4. Venetoclax in Adult Hematology

{kind=link}
| Date | Approval | References |
|---|---|---|
| 11 April 2016 | For the treatment of patients with CLL with a 17p deletion, as detected with an FDA-approved test, who have received at least one prior therapy | [39] |
| 8 June 2018 | In combination with rituximab for the treatment of people with CLL or SLL, with or without a 17p deletion, who have received at least one prior therapy | [24] |
| 21 November 2018 | Accelerated approval to venetoclax, in combination with azacitidine or decitabine or low-dose cytarabine for the treatment of newly diagnosed AML in adults who are age 75 years or older, or who have comorbidities that preclude the use of intensive induction chemotherapy | [40] |
| 15 May 2019 | In combination with obinutuzumab for previously untreated patients with CLL or SLL | [25] |
| 16 October 2020 | Full approval of venetoclax in combination with azacitidine, decitabine, or low-dose cytarabine (LDAC) for the treatment of newly diagnosed AML in adults 75 years or older, or who have comorbidities that preclude the use of intensive induction chemotherapy | [26] |
2. Pediatric AML
2.1. Clinical Studies in Relapsed/Refractory AML
2.2. Other Studies on Venetoclax Combination Therapies in AML
2.3. Genetic Sensitivity and Resistance to Venetoclax
3. Pediatric ALL
3.1. Comprehensive Treatment with Venetoclax
3.2. Venetoclax in Current Clinical Trials
3.3. Other Studies on Venetoclax Combination Therapies in ALL
4. The Mechanisms of Venetoclax Resistance and Future Strategies
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Voss, A.K.; Strasser, A. The Essentials of Developmental Apoptosis. F1000Research 2020, 9. [Google Scholar] [CrossRef] [PubMed]
- Thompson, C.B. Apoptosis in the Pathogenesis and Treatment of Disease. Science 1995, 267, 1456–1462. [Google Scholar] [CrossRef] [PubMed]
- Bertheloot, D.; Latz, E.; Franklin, B.S. Necroptosis, Pyroptosis and Apoptosis: An Intricate Game of Cell Death. Cell. Mol. Immunol. 2021, 18, 1106–1121. [Google Scholar] [CrossRef] [PubMed]
- Galluzzi, L.; Vitale, I.; Aaronson, S.A.; Abrams, J.M.; Adam, D.; Agostinis, P.; Alnemri, E.S.; Altucci, L.; Amelio, I.; Andrews, D.W.; et al. Molecular Mechanisms of Cell Death: Recommendations of the Nomenclature Committee on Cell Death 2018. Cell Death Differ. 2018, 25, 486–541. [Google Scholar] [CrossRef] [PubMed]
- Lomonosova, E.; Chinnadurai, G. BH3-Only Proteins in Apoptosis and beyond: An Overview. Oncogene 2008, 27 (Suppl. S1), S2–S19. [Google Scholar] [CrossRef] [PubMed]
- Pistritto, G.; Trisciuoglio, D.; Ceci, C.; Garufi, A.; D’Orazi, G. Apoptosis as Anticancer Mechanism: Function and Dysfunction of Its Modulators and Targeted Therapeutic Strategies. Aging 2016, 8, 603–619. [Google Scholar] [CrossRef]
- Czabotar, P.E.; Lessene, G.; Strasser, A.; Adams, J.M. Control of Apoptosis by the BCL-2 Protein Family: Implications for Physiology and Therapy. Nat. Rev. Mol. Cell Biol. 2014, 15, 49–63. [Google Scholar] [CrossRef]
- Warren, C.F.A.; Wong-Brown, M.W.; Bowden, N.A. BCL-2 Family Isoforms in Apoptosis and Cancer. Cell Death Dis. 2019, 10, 177. [Google Scholar] [CrossRef] [PubMed]
- Shamas-Din, A.; Kale, J.; Leber, B.; Andrews, D.W. Mechanisms of Action of Bcl-2 Family Proteins. Cold Spring Harb. Perspect. Biol. 2013, 5, a008714. [Google Scholar] [CrossRef]
- Kuwana, T.; Bouchier-Hayes, L.; Chipuk, J.E.; Bonzon, C.; Sullivan, B.A.; Green, D.R.; Newmeyer, D.D. BH3 Domains of BH3-Only Proteins Differentially Regulate Bax-Mediated Mitochondrial Membrane Permeabilization Both Directly and Indirectly. Mol. Cell 2005, 17, 525–535. [Google Scholar] [CrossRef]
- Cheng, E.H.; Wei, M.C.; Weiler, S.; Flavell, R.A.; Mak, T.W.; Lindsten, T.; Korsmeyer, S.J. BCL-2, BCL-X(L) Sequester BH3 Domain-Only Molecules Preventing BAX- and BAK-Mediated Mitochondrial Apoptosis. Mol. Cell 2001, 8, 705–711. [Google Scholar] [CrossRef]
- Senichkin, V.V.; Pervushin, N.V.; Zuev, A.P.; Zhivotovsky, B.; Kopeina, G.S. Targeting Bcl-2 Family Proteins: What, Where, When? Biochemistry 2020, 85, 1210–1226. [Google Scholar] [CrossRef] [PubMed]
- Souers, A.J.; Leverson, J.D.; Boghaert, E.R.; Ackler, S.L.; Catron, N.D.; Chen, J.; Dayton, B.D.; Ding, H.; Enschede, S.H.; Fairbrother, W.J.; et al. ABT-199, a Potent and Selective BCL-2 Inhibitor, Achieves Antitumor Activity While Sparing Platelets. Nat. Med. 2013, 19, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Tse, C.; Shoemaker, A.R.; Adickes, J.; Anderson, M.G.; Chen, J.; Jin, S.; Johnson, E.F.; Marsh, K.C.; Mitten, M.J.; Nimmer, P.; et al. ABT-263: A Potent and Orally Bioavailable Bcl-2 Family Inhibitor. Cancer Res. 2008, 68, 3421–3428. [Google Scholar] [CrossRef] [PubMed]
- Park, C.-M.; Bruncko, M.; Adickes, J.; Bauch, J.; Ding, H.; Kunzer, A.; Marsh, K.C.; Nimmer, P.; Shoemaker, A.R.; Song, X.; et al. Discovery of an Orally Bioavailable Small Molecule Inhibitor of Prosurvival B-Cell Lymphoma 2 Proteins. J. Med. Chem. 2008, 51, 6902–6915. [Google Scholar] [CrossRef] [PubMed]
- Oltersdorf, T.; Elmore, S.W.; Shoemaker, A.R.; Armstrong, R.C.; Augeri, D.J.; Belli, B.A.; Bruncko, M.; Deckwerth, T.L.; Dinges, J.; Hajduk, P.J.; et al. An Inhibitor of Bcl-2 Family Proteins Induces Regression of Solid Tumours. Nature 2005, 435, 677–681. [Google Scholar] [CrossRef]
- Konopleva, M.; Watt, J.; Contractor, R.; Tsao, T.; Harris, D.; Estrov, Z.; Bornmann, W.; Kantarjian, H.; Viallet, J.; Samudio, I.; et al. Mechanisms of Antileukemic Activity of the Novel Bcl-2 Homology Domain-3 Mimetic GX15-070 (Obatoclax). Cancer Res. 2008, 68, 3413–3420. [Google Scholar] [CrossRef]
- Trudel, S.; Li, Z.H.; Rauw, J.; Tiedemann, R.E.; Wen, X.Y.; Stewart, A.K. Preclinical Studies of the Pan-Bcl Inhibitor Obatoclax (GX015-070) in Multiple Myeloma. Blood 2007, 109, 5430–5438. [Google Scholar] [CrossRef]
- Urtishak, K.A.; Edwards, A.Y.Z.; Wang, L.-S.; Hudome, A.; Robinson, B.W.; Barrett, J.S.; Cao, K.; Cory, L.; Moore, J.S.; Bantly, A.D.; et al. Potent Obatoclax Cytotoxicity and Activation of Triple Death Mode Killing across Infant Acute Lymphoblastic Leukemia. Blood 2013, 121, 2689–2703. [Google Scholar] [CrossRef]
- Goard, C.A.; Schimmer, A.D. An Evidence-Based Review of Obatoclax Mesylate in the Treatment of Hematological Malignancies. Core Evid. 2013, 8, 15–26. [Google Scholar] [CrossRef]
- Han, Z.; Liang, J.; Li, Y.; He, J. Drugs and Clinical Approaches Targeting the Antiapoptotic Protein: A Review. BioMed Res. Int. 2019, 2019, 1212369. [Google Scholar] [CrossRef] [PubMed]
- Guerra, V.A.; DiNardo, C.; Konopleva, M. Venetoclax-Based Therapies for Acute Myeloid Leukemia. Best Pract. Res. Clin. Haematol. 2019, 32, 145–153. [Google Scholar] [CrossRef]
- VENCLEXTA (Venetoclax Tablets) Prescribing Information. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/208573s009lbl.pdf (accessed on 10 October 2023).
- US Food and Drug Administration. FDA Approves Venetoclax for CLL or SLL, with or without 17 p Deletion, after One Prior Therapy. Available online: https://www.fda.gov/drugs/informationondrugs/approveddrugs/ucm610308.htm (accessed on 10 October 2023).
- US Food and Drug Administration. FDA Approves Venetoclax for CLL and SLL. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-venetoclax-cll-and-sll (accessed on 10 October 2023).
- US Food and Drug Administration. FDA Approves Venetoclax in Combination for AML in Adults. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-grants-regular-approval-venetoclax-combination-untreated-acute-myeloid-leukemia (accessed on 10 October 2023).
- Konopleva, M.; Pollyea, D.A.; Potluri, J.; Chyla, B.; Hogdal, L.; Busman, T.; McKeegan, E.; Salem, A.H.; Zhu, M.; Ricker, J.L.; et al. Efficacy and Biological Correlates of Response in a Phase II Study of Venetoclax Monotherapy in Patients with Acute Myelogenous Leukemia. Cancer Discov. 2016, 6, 1106–1117. [Google Scholar] [CrossRef]
- DiNardo, C.D.; Pratz, K.W.; Letai, A.; Jonas, B.A.; Wei, A.H.; Thirman, M.; Arellano, M.; Frattini, M.G.; Kantarjian, H.; Popovic, R.; et al. Safety and Preliminary Efficacy of Venetoclax with Decitabine or Azacitidine in Elderly Patients with Previously Untreated Acute Myeloid Leukaemia: A Non-Randomised, Open-Label, Phase 1b Study. Lancet Oncol. 2018, 19, 216–228. [Google Scholar] [CrossRef]
- DiNardo, C.D.; Pratz, K.; Pullarkat, V.; Jonas, B.A.; Arellano, M.; Becker, P.S.; Frankfurt, O.; Konopleva, M.; Wei, A.H.; Kantarjian, H.M.; et al. Venetoclax Combined with Decitabine or Azacitidine in Treatment-Naive, Elderly Patients with Acute Myeloid Leukemia. Blood 2019, 133, 7–17. [Google Scholar] [CrossRef]
- Wei, A.H.; Strickland, S.A.; Hou, J.-Z.; Fiedler, W.; Lin, T.L.; Walter, R.B.; Enjeti, A.; Tiong, I.S.; Savona, M.; Lee, S.; et al. Venetoclax Combined with Low-Dose Cytarabine for Previously Untreated Patients with Acute Myeloid Leukemia: Results from a Phase Ib/II Study. J. Clin. Oncol. 2019, 37, 1277–1284. [Google Scholar] [CrossRef] [PubMed]
- McMahon, C.M.; Ferng, T.; Canaani, J.; Wang, E.S.; Morrissette, J.J.D.; Eastburn, D.J.; Pellegrino, M.; Durruthy-Durruthy, R.; Watt, C.D.; Asthana, S.; et al. Clonal Selection with RAS Pathway Activation Mediates Secondary Clinical Resistance to Selective FLT3 Inhibition in Acute Myeloid Leukemia. Cancer Discov. 2019, 9, 1050–1063. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Maiti, A.; Kadia, T.M.; Ravandi, F.; Daver, N.; Pemmaraju, N.; Borthakur, G.; Bose, P.; Issa, G.C.; Short, N.J.; et al. Outcomes of TP53-Mutant Acute Myeloid Leukemia with Venetoclax and Decitabine. Blood 2020, 136, 33–36. [Google Scholar] [CrossRef]
- Seymour, J.F.; Ma, S.; Brander, D.M.; Choi, M.Y.; Barrientos, J.; Davids, M.S.; Anderson, M.A.; Beaven, A.W.; Rosen, S.T.; Tam, C.S.; et al. Venetoclax plus Rituximab in Relapsed or Refractory Chronic Lymphocytic Leukaemia: A Phase 1b Study. Lancet Oncol. 2017, 18, 230–240. [Google Scholar] [CrossRef]
- Anderson, M.A.; Deng, J.; Seymour, J.F.; Tam, C.; Kim, S.Y.; Fein, J.; Yu, L.; Brown, J.R.; Westerman, D.; Si, E.G.; et al. The BCL2 Selective Inhibitor Venetoclax Induces Rapid Onset Apoptosis of CLL Cells in Patients via a TP53-Independent Mechanism. Blood 2016, 127, 3215–3224. [Google Scholar] [CrossRef]
- Roberts, A.W.; Davids, M.S.; Pagel, J.M.; Kahl, B.S.; Puvvada, S.D.; Gerecitano, J.F.; Kipps, T.J.; Anderson, M.A.; Brown, J.R.; Gressick, L.; et al. Targeting BCL2 with Venetoclax in Relapsed Chronic Lymphocytic Leukemia. N. Engl. J. Med. 2016, 374, 311–322. [Google Scholar] [CrossRef]
- Stilgenbauer, S.; Eichhorst, B.; Schetelig, J.; Hillmen, P.; Seymour, J.F.; Coutre, S.; Jurczak, W.; Mulligan, S.P.; Schuh, A.; Assouline, S.; et al. Venetoclax for Patients with Chronic Lymphocytic Leukemia with 17p Deletion: Results from the Full Population of a Phase II Pivotal Trial. J. Clin. Oncol. 2018, 36, 1973–1980. [Google Scholar] [CrossRef]
- Mato, A.R.; Hill, B.T.; Lamanna, N.; Barr, P.M.; Ujjani, C.S.; Brander, D.M.; Howlett, C.; Skarbnik, A.P.; Cheson, B.D.; Zent, C.S.; et al. Optimal Sequencing of Ibrutinib, Idelalisib, and Venetoclax in Chronic Lymphocytic Leukemia: Results from a Multicenter Study of 683 Patients. Ann. Oncol. 2017, 28, 1050–1056. [Google Scholar] [CrossRef] [PubMed]
- Hillmen, P.; Rawstron, A.C.; Brock, K.; Muñoz-Vicente, S.; Yates, F.J.; Bishop, R.; Boucher, R.; MacDonald, D.; Fegan, C.; McCaig, A.; et al. Ibrutinib Plus Venetoclax in Relapsed/Refractory Chronic Lymphocytic Leukemia: The CLARITY Study. J. Clin. Oncol. 2019, 37, 2722–2729. [Google Scholar] [CrossRef] [PubMed]
- Food and Drug Administration. Approved Drugs Venetoclax (Venclexta) Tablets. Available online: http://www.fda.gov/Drugs/InformationOnDrugs/ApprovedDrugs/ucm495351.htm (accessed on 12 November 2023).
- US Food and Drug Administration. FDA Grants Regular Approval to Venetoclax in Combination for Untreated Acute Myeloid Leukemia. Available online: https://www.fda.gov/drugs/fda-approves-venetoclax-combination-aml-adults (accessed on 12 November 2023).
- Ascentage Pharma. Ascentage Pharma Received Clearance from U.S. FDA to Proceed with Global Registrational Phase III Clinical Trial for Lisaftoclax (APG-2575) in Previously Treated Patients with CLL/SLL. Available online: https://ascentage.com/ascentage-pharma-received-clearance-from-u-s-fda-to-proceed-with-global-registrational-phase-iii-clinical-trial-for-lisaftoclax-apg-2575-in-previously-treated-patients-with-cll-sll/ (accessed on 12 November 2023).
- Ascentage Pharma. Ascentage Pharma Announces Its 9th Orphan Drug Designation from the US FDA in 2020, Setting a Record for Chinese Biopharmaceutical Companies. Available online: https://ascentage.com/ascentage-pharma-announces-its-9th-orphan-drug-designation-from-the-us-fda-in-2020-setting-a-record-for-chinese-biopharmaceutical-companies/ (accessed on 12 November 2023).
- Hunger, S.P.; Raetz, E.A. How I Treat Relapsed Acute Lymphoblastic Leukemia in the Pediatric Population. Blood 2020, 136, 1803–1812. [Google Scholar] [CrossRef] [PubMed]
- Zarnegar-Lumley, S.; Caldwell, K.J.; Rubnitz, J.E. Relapsed Acute Myeloid Leukemia in Children and Adolescents: Current Treatment Options and Future Strategies. Leukemia 2022, 36, 1951–1960. [Google Scholar] [CrossRef]
- Rasche, M.; Zimmermann, M.; Steidel, E.; Alonzo, T.; Aplenc, R.; Bourquin, J.-P.; Boztug, H.; Cooper, T.; Gamis, A.S.; Gerbing, R.B.; et al. Survival Following Relapse in Children with Acute Myeloid Leukemia: A Report from AML-BFM and COG. Cancers 2021, 13, 2336. [Google Scholar] [CrossRef]
- Bradbury, D.A.; Zhu, Y.M.; Russell, N.H. Bcl-2 Expression in Acute Myeloblastic Leukaemia: Relationship with Autonomous Growth and CD34 Antigen Expression. Leuk Lymphoma 1997, 24, 221–228. [Google Scholar] [CrossRef]
- Bensi, L.; Longo, R.; Vecchi, A.; Messora, C.; Garagnani, L.; Bernardi, S.; Tamassia, M.G.; Sacchi, S. Bcl-2 Oncoprotein Expression in Acute Myeloid Leukemia. Haematologica 1995, 80, 98–102. [Google Scholar]
- Pan, R.; Hogdal, L.J.; Benito, J.M.; Bucci, D.; Han, L.; Borthakur, G.; Cortes, J.; DeAngelo, D.J.; Debose, L.; Mu, H.; et al. Selective BCL-2 Inhibition by ABT-199 Causes on-Target Cell Death in Acute Myeloid Leukemia. Cancer Discov. 2014, 4, 362–375. [Google Scholar] [CrossRef]
- Bogenberger, J.M.; Kornblau, S.M.; Pierceall, W.E.; Lena, R.; Chow, D.; Shi, C.-X.; Mantei, J.; Ahmann, G.; Gonzales, I.M.; Choudhary, A.; et al. BCL-2 Family Proteins as 5-Azacytidine-Sensitizing Targets and Determinants of Response in Myeloid Malignancies. Leukemia 2014, 28, 1657–1665. [Google Scholar] [CrossRef] [PubMed]
- DiNardo, C.D.; Maiti, A.; Rausch, C.R.; Pemmaraju, N.; Naqvi, K.; Daver, N.G.; Kadia, T.M.; Borthakur, G.; Ohanian, M.; Alvarado, Y.; et al. 10-Day Decitabine with Venetoclax for Newly Diagnosed Intensive Chemotherapy Ineligible, and Relapsed or Refractory Acute Myeloid Leukaemia: A Single-Centre, Phase 2 Trial. Lancet Haematol. 2020, 7, e724–e736. [Google Scholar] [CrossRef] [PubMed]
- Karol, S.E.; Alexander, T.B.; Budhraja, A.; Pounds, S.B.; Canavera, K.; Wang, L.; Wolf, J.; Klco, J.M.; Mead, P.E.; Gupta, S.D.; et al. Venetoclax in Combination with Cytarabine with or without Idarubicin in Children with Relapsed or Refractory Acute Myeloid Leukaemia: A Phase 1, Dose-Escalation Study. Lancet Oncol. 2020, 21, 551–560. [Google Scholar] [CrossRef] [PubMed]
- Place, A.E.; Goldsmith, K.; Bourquin, J.-P.; Loh, M.L.; Gore, L.; Morgenstern, D.A.; Sanzgiri, Y.; Hoffman, D.; Zhou, Y.; Ross, J.A.; et al. Accelerating Drug Development in Pediatric Cancer: A Novel Phase I Study Design of Venetoclax in Relapsed/Refractory Malignancies. Future Oncol. 2018, 14, 2115–2129. [Google Scholar] [CrossRef] [PubMed]
- Gonzales, F.; Guilmatre, A.; Barthélémy, A.; Lapillonne, H.; Pottier, N.; Leverger, G.; Petit, A.; Cheok, M.H. Ex Vivo Drug Sensitivity Profiling-Guided Treatment of a Relapsed Pediatric Mixed-Phenotype Acute Leukemia with Venetoclax and Azacitidine. Pediatr. Blood Cancer 2022, 69, e29678. [Google Scholar] [CrossRef] [PubMed]
- Mishra, A.K.; Mullanfiroze, K.; Chiesa, R.; Vora, A. Azacitidine and Venetoclax for Post-Transplant Relapse in a Case of CBFA2T3/GLIS2 Childhood Acute Myeloid Leukaemia. Pediatr. Blood Cancer 2021, 68, e29221. [Google Scholar] [CrossRef] [PubMed]
- Wen, X.; Wu, Y.; Huang, P.; Zheng, H. Combined Treatment with Venetoclax, Dasatinib, and FLT3 Inhibitors for NUP98-NSD1+/FLT3-ITD+ Acute Myeloid Leukemia: A Pediatric Case Report. Pediatr. Blood Cancer 2023, 70, e30308. [Google Scholar] [CrossRef]
- Xu, H.; Yu, H.; Xu, J.; Zhou, F.; Tang, S.; Feng, X.; Luo, Q.; Zhang, B.; Wu, X.; Jin, R.; et al. Refractory Pediatric Acute Myeloid Leukemia Expressing NUP98-NSD1 Fusion Gene Responsive to Chemotherapy Combined with Venetoclax and Decitabine. Pediatr. Blood Cancer 2023, 70, e30021. [Google Scholar] [CrossRef]
- Naviglio, S.; Grasso, A.G.; Iacono, C.; Zanella, G.; Kiren, V.; Giurici, N.; Verzegnassi, F.; Maximova, N.; Rabusin, M. Case Report: Venetoclax Therapy in a Boy with Acute Myeloid Leukemia in Shwachman Diamond Syndrome. Front. Pediatr. 2022, 10, 1059569. [Google Scholar] [CrossRef]
- Wen, X.; Yu, J.; Fan, J.; Zhu, S.; Zheng, H. Case Report: Positive Response to Venetoclax and Azacitidine in the Treatment of Acute Myeloid Leukemia with Myelodysplasia-Related Changes and Blasts of the Mixed T/Myeloid Phenotype. Pediatr. Blood Cancer 2023, 70, e30597. [Google Scholar] [CrossRef]
- Ma, J.; Morimoto, K.; Pulsipher, M.A.; Parekh, C. Venetoclax and Azacitidine in the Treatment of NPM1-Mutated Donor Cell–Derived Leukemia in a Patient with Fanconi Anemia: Case Report and Literature Review. JCO Precis. Oncol. 2023, 7, e2200693. [Google Scholar] [CrossRef] [PubMed]
- Pfeiffer, T.; Li, Y.; Ashcraft, E.; Karol, S.E.; Rubnitz, J.E.; Epperly, R.; Madden, R.; Mamcarz, E.; Obeng, E.; Qudeimat, A.; et al. Venetoclax-Based Therapy as a Bridge to Allogeneic Hematopoietic Cell Transplantation in Children with Relapsed/Refractory AML. Bone Marrow Transplant. 2023, 58, 328–331. [Google Scholar] [CrossRef] [PubMed]
- Niswander, L.M.; Chung, P.; Diorio, C.; Tasian, S.K. Clinical Responses in Pediatric Patients with Relapsed/Refractory Leukemia Treated with Azacitidine and Venetoclax. Haematologica 2020, 108, 3142. [Google Scholar] [CrossRef] [PubMed]
- Masetti, R.; Baccelli, F.; Leardini, D.; Gottardi, F.; Vendemini, F.; Di Gangi, A.; Becilli, M.; Lodi, M.; Tumino, M.; Vinci, L.; et al. Venetoclax-Based Therapies in Pediatric Advanced MDS and Relapsed/Refractory AML: A Multicenter Retrospective Analysis. Blood Adv. 2023, 7, 4366–4370. [Google Scholar] [CrossRef] [PubMed]
- Winters, A.C.; Maloney, K.W.; Treece, A.L.; Gore, L.; Franklin, A.K. Single-Center Pediatric Experience with Venetoclax and Azacitidine as Treatment for Myelodysplastic Syndrome and Acute Myeloid Leukemia. Pediatr. Blood Cancer 2020, 67, e28398. [Google Scholar] [CrossRef] [PubMed]
- Bobeff, K.; Pastorczak, A.; Urbanska, Z.; Balwierz, W.; Juraszewska, E.; Wachowiak, J.; Derwich, K.; Samborska, M.; Kalwak, K.; Dachowska-Kalwak, I.; et al. Venetoclax Use in Paediatric Haemato-Oncology Centres in Poland: A 2022 Survey. Children 2023, 10, 745. [Google Scholar] [CrossRef]
- Trabal, A.; Gibson, A.; He, J.; McCall, D.; Roth, M.; Nuñez, C.; Garcia, M.; Buzbee, M.; Toepfer, L.; Bidikian, A.; et al. Venetoclax for Acute Myeloid Leukemia in Pediatric Patients: A Texas Medical Center Experience. Cancers 2023, 15, 1983. [Google Scholar] [CrossRef]
- Marinoff, A.E.; Aaronson, K.; Agrawal, A.K.; Braun, B.S.; Golden, C.; Huang, B.J.; Michlitsch, J.; Southworth, E.; Thrall, A.; Vo, K.T.; et al. Venetoclax in Combination with Chemotherapy as Treatment for Pediatric Advanced Hematologic Malignancies. Pediatr. Blood Cancer 2023, 70, e30335. [Google Scholar] [CrossRef]
- Conneely, S.E.; Rau, R.E. The Genomics of Acute Myeloid Leukemia in Children. Cancer Metastasis Rev. 2020, 39, 189–209. [Google Scholar] [CrossRef]
- Zafar, N.; Ghias, K.; Fadoo, Z. Genetic Aberrations Involved in Relapse of Pediatric Acute Myeloid Leukemia: A Literature Review. Asia-Pac. J. Clin. Oncol. 2021, 17, e135–e141. [Google Scholar] [CrossRef]
- Winters, A.C.; Bernt, K.M. MLL-Rearranged Leukemias-An Update on Science and Clinical Approaches. Front. Pediatr. 2017, 5, 4. [Google Scholar] [CrossRef] [PubMed]
- Meyer, C.; Burmeister, T.; Gröger, D.; Tsaur, G.; Fechina, L.; Renneville, A.; Sutton, R.; Venn, N.C.; Emerenciano, M.; Pombo-de-Oliveira, M.S.; et al. The MLL Recombinome of Acute Leukemias in 2017. Leukemia 2018, 32, 273–284. [Google Scholar] [CrossRef]
- Creutzig, U.; Zimmermann, M.; Reinhardt, D.; Rasche, M.; von Neuhoff, C.; Alpermann, T.; Dworzak, M.; Perglerová, K.; Zemanova, Z.; Tchinda, J.; et al. Changes in Cytogenetics and Molecular Genetics in Acute Myeloid Leukemia from Childhood to Adult Age Groups. Cancer 2016, 122, 3821–3830. [Google Scholar] [CrossRef]
- Harrison, C.J.; Hills, R.K.; Moorman, A.V.; Grimwade, D.J.; Hann, I.; Webb, D.K.H.; Wheatley, K.; de Graaf, S.S.N.; van den Berg, E.; Burnett, A.K.; et al. Cytogenetics of Childhood Acute Myeloid Leukemia: United Kingdom Medical Research Council Treatment Trials AML 10 and 12. J. Clin. Oncol. 2010, 28, 2674–2681. [Google Scholar] [CrossRef] [PubMed]
- Cheung, L.C.; Aya-Bonilla, C.; Cruickshank, M.N.; Chiu, S.K.; Kuek, V.; Anderson, D.; Chua, G.-A.; Singh, S.; Oommen, J.; Ferrari, E.; et al. Preclinical Efficacy of Azacitidine and Venetoclax for Infant KMT2A-Rearranged Acute Lymphoblastic Leukemia Reveals a New Therapeutic Strategy. Leukemia 2023, 37, 61. [Google Scholar] [CrossRef] [PubMed]
- Tregnago, C.; Benetton, M.; Da Ros, A.; Borella, G.; Longo, G.; Polato, K.; Francescato, S.; Biffi, A.; Pigazzi, M. Novel Compounds Synergize with Venetoclax to Target KMT2A-Rearranged Pediatric Acute Myeloid Leukemia. Front. Pharmacol. 2022, 12, 820191. [Google Scholar] [CrossRef]
- Ball, B.J.; Arslan, S.; Koller, P.; Ngo, D.; Afkhami, M.; Salhotra, A.; Al-Malki, M.; Aribi, A.; Ali, H.; Sandhu, K.; et al. Clinical Experience with Venetoclax and Hypomethylating Agents (HMA) in Patients with Newly Diagnosed and Relapsed or Refractory KMT2A-Rearranged Acute Myeloid Leukemia (AML). Leuk. Lymphoma 2022, 63, 3232–3236. [Google Scholar] [CrossRef]
- Bisaillon, R.; Moison, C.; Thiollier, C.; Krosl, J.; Bordeleau, M.-E.; Lehnertz, B.; Lavallée, V.-P.; MacRae, T.; Mayotte, N.; Labelle, C.; et al. Genetic Characterization of ABT-199 Sensitivity in Human AML. Leukemia 2020, 34, 63–74. [Google Scholar] [CrossRef]
- Griffioen, M.S.; de Leeuw, D.C.; Janssen, J.J.W.M.; Smit, L. Targeting Acute Myeloid Leukemia with Venetoclax; Biomarkers for Sensitivity and Rationale for Venetoclax-Based Combination Therapies. Cancers 2022, 14, 3456. [Google Scholar] [CrossRef]
- Lachowiez, C.A.; Loghavi, S.; Kadia, T.M.; Daver, N.; Borthakur, G.; Pemmaraju, N.; Naqvi, K.; Alvarado, Y.; Yilmaz, M.; Short, N.; et al. Outcomes of Older Patients with NPM1-Mutated AML: Current Treatments and the Promise of Venetoclax-Based Regimens. Blood Adv. 2020, 4, 1311–1320. [Google Scholar] [CrossRef]
- Hollink, I.H.I.M.; Zwaan, C.M.; Zimmermann, M.; Arentsen-Peters, T.C.J.M.; Pieters, R.; Cloos, J.; Kaspers, G.J.L.; de Graaf, S.S.N.; Harbott, J.; Creutzig, U.; et al. Favorable Prognostic Impact of NPM1 Gene Mutations in Childhood Acute Myeloid Leukemia, with Emphasis on Cytogenetically Normal AML. Leukemia 2009, 23, 262–270. [Google Scholar] [CrossRef] [PubMed]
- Brown, P.; McIntyre, E.; Rau, R.; Meshinchi, S.; Lacayo, N.; Dahl, G.; Alonzo, T.A.; Chang, M.; Arceci, R.J.; Small, D. The Incidence and Clinical Significance of Nucleophosmin Mutations in Childhood AML. Blood 2007, 110, 979–985. [Google Scholar] [CrossRef] [PubMed]
- Stevens, B.M.; Jones, C.L.; Winters, A.; Dugan, J.; Abbott, D.; Savona, M.R.; Fesik, S.W.; Pollyea, D.A.; Jordan, C.T. PTPN11 Mutations Confer Unique Metabolic Properties and Increase Resistance to Venetoclax and Azacitidine in Acute Myelogenous Leukemia. Blood 2018, 132, 909. [Google Scholar] [CrossRef]
- Bolouri, H.; Farrar, J.E.; Triche, T.; Ries, R.E.; Lim, E.L.; Alonzo, T.A.; Ma, Y.; Moore, R.; Mungall, A.J.; Marra, M.A.; et al. The Molecular Landscape of Pediatric Acute Myeloid Leukemia Reveals Recurrent Structural Alterations and Age-Specific Mutational Interactions. Nat. Med. 2018, 24, 103–112. [Google Scholar] [CrossRef] [PubMed]
- Tarlock, K.; Alonzo, T.A.; Loken, M.R.; Gerbing, R.B.; Ries, R.E.; Aplenc, R.; Sung, L.; Raimondi, S.C.; Hirsch, B.A.; Kahwash, S.B.; et al. Disease Characteristics and Prognostic Implications of Cell Surface FLT3 Receptor (CD135) Expression in Pediatric Acute Myeloid Leukemia: A Report from the Children’s Oncology Group. Clin. Cancer Res. 2017, 23, 3649–3656. [Google Scholar] [CrossRef] [PubMed]
- Chyla, B.; Daver, N.; Doyle, K.; McKeegan, E.; Huang, X.; Ruvolo, V.; Wang, Z.; Chen, K.; Souers, A.; Leverson, J.; et al. Genetic Biomarkers of Sensitivity and Resistance to Venetoclax Monotherapy in Patients with Relapsed Acute Myeloid Leukemia. Am. J. Hematol. 2018, 93, E202–E205. [Google Scholar] [CrossRef]
- Perl, A.E.; Martinelli, G.; Cortes, J.E.; Neubauer, A.; Berman, E.; Paolini, S.; Montesinos, P.; Baer, M.R.; Larson, R.A.; Ustun, C.; et al. Gilteritinib or Chemotherapy for Relapsed or Refractory FLT3-Mutated AML. N. Engl. J. Med. 2019, 381, 1728–1740. [Google Scholar] [CrossRef]
- Daver, N.; Perl, A.E.; Maly, J.; Levis, M.; Ritchie, E.; Litzow, M.; McCloskey, J.; Smith, C.C.; Schiller, G.; Bradley, T.; et al. Venetoclax Plus Gilteritinib for FLT3-Mutated Relapsed/Refractory Acute Myeloid Leukemia. J. Clin. Oncol. 2022, 40, 4048–4059. [Google Scholar] [CrossRef]
- Smith, S.M.; Lee, A.; Tong, S.; Leung, S.; Hongo, H.; Rivera, J.; Sweet-Cordero, A.; Michlitsch, J.; Stieglitz, E. Detection of a GLIS3 Fusion in an Infant with AML Refractory to Chemotherapy. Cold Spring Harb. Perspect. Biol. 2022, 8, a006220. [Google Scholar] [CrossRef]
- Smith, J.L.; Ries, R.E.; Hylkema, T.; Alonzo, T.A.; Gerbing, R.B.; Santaguida, M.T.; Eidenschink Brodersen, L.; Pardo, L.; Cummings, C.L.; Loeb, K.R.; et al. Comprehensive Transcriptome Profiling of Cryptic CBFA2T3-GLIS2 Fusion-Positive AML Defines Novel Therapeutic Options: A COG and TARGET Pediatric AML Study. Clin. Cancer Res. 2020, 26, 726–737. [Google Scholar] [CrossRef]
- Gress, V.; Roussy, M.; Boulianne, L.; Bilodeau, M.; Cardin, S.; El-Hachem, N.; Lisi, V.; Khakipoor, B.; Rouette, A.; Farah, A.; et al. CBFA2T3::GLIS2 Pediatric Acute Megakaryoblastic Leukemia Is Sensitive to BCL-XL Inhibition by Navitoclax and DT2216. Blood Adv. 2023. [Google Scholar] [CrossRef] [PubMed]
- Hunger, S.P.; Lu, X.; Devidas, M.; Camitta, B.M.; Gaynon, P.S.; Winick, N.J.; Reaman, G.H.; Carroll, W.L. Improved Survival for Children and Adolescents with Acute Lymphoblastic Leukemia between 1990 and 2005: A Report from the Children’s Oncology Group. J. Clin. Oncol. 2012, 30, 1663–1669. [Google Scholar] [CrossRef]
- Richter, A.; Fischer, E.; Holz, C.; Schulze, J.; Lange, S.; Sekora, A.; Knuebel, G.; Henze, L.; Roolf, C.; Murua Escobar, H.; et al. Combined Application of Pan-AKT Inhibitor MK-2206 and BCL-2 Antagonist Venetoclax in B-Cell Precursor Acute Lymphoblastic Leukemia. Int. J. Mol. Sci. 2021, 22, 2771. [Google Scholar] [CrossRef]
- Canaani, J.; Frisch, A.; Pollyea, D.A.; Schwartz, M.; Aumann, S.; Ganzel, C.; Haran, A.; Even-Zohar, N.G.; Shaulov, A.; Vainstein, V.; et al. Venetoclax-Based Salvage Therapy for Adult Patients with Relapsed/Refractory Acute Lymphoblastic Leukemia. Eur. J. Haematol. 2023, 111, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Holz, C.; Lange, S.; Sekora, A.; Knuebel, G.; Krohn, S.; Murua Escobar, H.; Junghanss, C.; Richter, A. Combined BCL-2 and PI3K/AKT Pathway Inhibition in KMT2A-Rearranged Acute B-Lymphoblastic Leukemia Cells. Int. J. Mol. Sci. 2023, 24, 1359. [Google Scholar] [CrossRef] [PubMed]
- Gibson, A.; Trabal, A.; McCall, D.; Khazal, S.; Toepfer, L.; Bell, D.H.; Roth, M.; Mahadeo, K.M.; Nunez, C.; Short, N.J.; et al. Venetoclax for Children and Adolescents with Acute Lymphoblastic Leukemia and Lymphoblastic Lymphoma. Cancers 2021, 14, 150. [Google Scholar] [CrossRef]
- Richard-Carpentier, G.; Jabbour, E.; Short, N.J.; Rausch, C.R.; Savoy, J.M.; Bose, P.; Yilmaz, M.; Jain, N.; Borthakur, G.; Ohanian, M.; et al. Clinical Experience with Venetoclax Combined with Chemotherapy for Relapsed or Refractory T-Cell Acute Lymphoblastic Leukemia. Clin. Lymphoma Myeloma Leuk. 2020, 20, 212–218. [Google Scholar] [CrossRef]
- Pullarkat, V.A.; Lacayo, N.J.; Jabbour, E.; Rubnitz, J.E.; Bajel, A.; Laetsch, T.W.; Leonard, J.; Colace, S.I.; Khaw, S.L.; Fleming, S.A.; et al. Venetoclax and Navitoclax in Combination with Chemotherapy in Patients with Relapsed or Refractory Acute Lymphoblastic Leukemia and Lymphoblastic Lymphoma. Cancer Discov. 2021, 11, 1440–1453. [Google Scholar] [CrossRef]
- Khaw, S.L.; Suryani, S.; Evans, K.; Richmond, J.; Robbins, A.; Kurmasheva, R.T.; Billups, C.A.; Erickson, S.W.; Guo, Y.; Houghton, P.J.; et al. Venetoclax Responses of Pediatric ALL Xenografts Reveal Sensitivity of MLL-Rearranged Leukemia. Blood 2016, 128, 1382–1395. [Google Scholar] [CrossRef]
- Diamanti, P.; Ede, B.C.; Dace, P.E.; Barendt, W.J.; Cox, C.V.; Hancock, J.P.; Moppett, J.P.; Blair, A. Investigating the Response of Paediatric Leukaemia-Propagating Cells to BCL-2 Inhibitors. Br. J. Haematol. 2021, 192, 577–588. [Google Scholar] [CrossRef]
- Brown, P.; Pieters, R.; Biondi, A. How I Treat Infant Leukemia. Blood 2019, 133, 205–214. [Google Scholar] [CrossRef]
- Pariury, H.; Fandel, J.; Bachl, S.; Ang, K.K.; Markossian, S.; Wilson, C.G.; Braun, B.S.; Popescu, B.; Wohlfeil, M.; Beckman, K.; et al. Venetoclax and Dinaciclib Elicit Synergistic Preclinical Efficacy against Hypodiploid Acute Lymphoblastic Leukemia. Haematologica 2023, 108, 1272–1283. [Google Scholar] [CrossRef]
- Summers, R.J.; Jain, J.; Vasileiadi, E.; Smith, B.; Chimenti, M.L.; Yeung, T.Y.; Kelvin, J.; Wang, X.; Frye, S.V.; Earp, H.S.; et al. Therapeutic Targeting of MERTK and BCL-2 in T-Cell and Early T-Precursor Acute Lymphoblastic Leukemia. Cancers 2022, 14, 6142. [Google Scholar] [CrossRef]
- Molina, J.C.; Asare, J.M.; Tuschong, L.; West, R.R.; Calvo, K.R.; Persky, R.; Boyce, A.M.; Hammoud, D.A.; Holland, S.M.; Hickstein, D.; et al. Venetoclax/Decitabine for a Pediatric Patient with Chronic Myelomonocytic Leukemia. Pediatr. Blood Cancer 2021, 68, e28865. [Google Scholar] [CrossRef] [PubMed]
- Abla, D.; Abboud, M.R.; Noun, D.; Tarek, N.; Pemmaraju, N. Hyper-CVAD Combined with Venetoclax for Relapsed Pediatric Blastic Plasmacytoid Dendritic Cell Neoplasm (BPDCN): A Case Report and Literature Review. Leuk. Res. Rep. 2022, 17, 100313. [Google Scholar] [CrossRef]
- Gottardi, F.; Baccelli, F.; Leardini, D.; Di Battista, A.; Castellucci, P.; D’Amico, D.; Serravalle, S.; Bertuccio, S.N.; Messelodi, D.; Prete, A.; et al. Successful Treatment of a Chemotherapy-Resistant t(17;19) Paediatric ALL with a Combination of Inotuzumab, Venetoclax and Navitoclax. Br. J. Haematol. 2023, 202, e39–e42. [Google Scholar] [CrossRef] [PubMed]
- Niu, X.; Zhao, J.; Ma, J.; Xie, C.; Edwards, H.; Wang, G.; Caldwell, J.T.; Xiang, S.; Zhang, X.; Chu, R.; et al. Binding of Released Bim to Mcl-1 Is a Mechanism of Intrinsic Resistance to ABT-199 Which Can Be Overcome by Combination with Daunorubicin or Cytarabine in AML Cells. Clin. Cancer Res. 2016, 22, 4440–4451. [Google Scholar] [CrossRef] [PubMed]
- Thijssen, R.; Roberts, A.W. Venetoclax in Lymphoid Malignancies: New Insights, More to Learn. Cancer Cell 2019, 36, 341–343. [Google Scholar] [CrossRef] [PubMed]
- Haselager, M.V.; Kielbassa, K.; Ter Burg, J.; Bax, D.J.C.; Fernandes, S.M.; Borst, J.; Tam, C.; Forconi, F.; Chiodin, G.; Brown, J.R.; et al. Changes in Bcl-2 Members after Ibrutinib or Venetoclax Uncover Functional Hierarchy in Determining Resistance to Venetoclax in CLL. Blood 2020, 136, 2918–2926. [Google Scholar] [CrossRef]
- Ashkenazi, A.; Fairbrother, W.J.; Leverson, J.D.; Souers, A.J. From Basic Apoptosis Discoveries to Advanced Selective BCL-2 Family Inhibitors. Nat. Rev. Drug Discov. 2017, 16, 273–284. [Google Scholar] [CrossRef]
- Agarwal, R.; Chan, Y.-C.; Tam, C.S.; Hunter, T.; Vassiliadis, D.; Teh, C.E.; Thijssen, R.; Yeh, P.; Wong, S.Q.; Ftouni, S.; et al. Dynamic Molecular Monitoring Reveals That SWI-SNF Mutations Mediate Resistance to Ibrutinib plus Venetoclax in Mantle Cell Lymphoma. Nat. Med. 2019, 25, 119–129. [Google Scholar] [CrossRef]
- Ma, J.; Zhao, S.; Qiao, X.; Knight, T.; Edwards, H.; Polin, L.; Kushner, J.; Dzinic, S.H.; White, K.; Wang, G.; et al. Inhibition of Bcl-2 Synergistically Enhances the Antileukemic Activity of Midostaurin and Gilteritinib in Preclinical Models of FLT3-Mutated Acute Myeloid Leukemia. Clin. Cancer Res. 2019, 25, 6815–6826. [Google Scholar] [CrossRef]
- Guièze, R.; Liu, V.M.; Rosebrock, D.; Jourdain, A.A.; Hernández-Sánchez, M.; Zurita, A.M.; Sun, J.; Hacken, E.T.; Baranowski, K.; Thompson, P.A.; et al. Mitochondrial Reprogramming Underlies Resistance to BCL-2 Inhibition in Lymphoid Malignancies. Cancer Cell 2019, 36, 369–384.e13. [Google Scholar] [CrossRef]
- Lin, K.H.; Winter, P.S.; Xie, A.; Roth, C.; Martz, C.A.; Stein, E.M.; Anderson, G.R.; Tingley, J.P.; Wood, K.C. Targeting MCL-1/BCL-XL Forestalls the Acquisition of Resistance to ABT-199 in Acute Myeloid Leukemia. Sci. Rep. 2016, 6, 27696. [Google Scholar] [CrossRef]
- Bose, P.; Gandhi, V.; Konopleva, M. Pathways and Mechanisms of Venetoclax Resistance. Leuk. Lymphoma 2017, 58, 2026–2039. [Google Scholar] [CrossRef]
- Tahir, S.K.; Smith, M.L.; Hessler, P.; Rapp, L.R.; Idler, K.B.; Park, C.H.; Leverson, J.D.; Lam, L.T. Potential Mechanisms of Resistance to Venetoclax and Strategies to Circumvent It. BMC Cancer 2017, 17, 399. [Google Scholar] [CrossRef] [PubMed]
- Schoenwaelder, S.M.; Jarman, K.E.; Gardiner, E.E.; Hua, M.; Qiao, J.; White, M.J.; Josefsson, E.C.; Alwis, I.; Ono, A.; Willcox, A.; et al. Bcl-xL-Inhibitory BH3 Mimetics Can Induce a Transient Thrombocytopathy That Undermines the Hemostatic Function of Platelets. Blood 2011, 118, 1663–1674. [Google Scholar] [CrossRef] [PubMed]
- Scherr, A.-L.; Mock, A.; Gdynia, G.; Schmitt, N.; Heilig, C.E.; Korell, F.; Rhadakrishnan, P.; Hoffmeister, P.; Metzeler, K.H.; Schulze-Osthoff, K.; et al. Identification of BCL-XL as Highly Active Survival Factor and Promising Therapeutic Target in Colorectal Cancer. Cell Death Dis. 2020, 11, 875. [Google Scholar] [CrossRef] [PubMed]
- Xiang, Z.; Luo, H.; Payton, J.E.; Cain, J.; Ley, T.J.; Opferman, J.T.; Tomasson, M.H. Mcl1 Haploinsufficiency Protects Mice from Myc-Induced Acute Myeloid Leukemia. J. Clin. Investig. 2010, 120, 2109–2118. [Google Scholar] [CrossRef]
- Teh, T.-C.; Nguyen, N.-Y.; Moujalled, D.M.; Segal, D.; Pomilio, G.; Rijal, S.; Jabbour, A.; Cummins, K.; Lackovic, K.; Blombery, P.; et al. Enhancing Venetoclax Activity in Acute Myeloid Leukemia by Co-Targeting MCL1. Leukemia 2018, 32, 303–312. [Google Scholar] [CrossRef]
- Kotschy, A.; Szlavik, Z.; Murray, J.; Davidson, J.; Maragno, A.L.; Le Toumelin-Braizat, G.; Chanrion, M.; Kelly, G.L.; Gong, J.-N.; Moujalled, D.M.; et al. The MCL1 Inhibitor S63845 Is Tolerable and Effective in Diverse Cancer Models. Nature 2016, 538, 477–482. [Google Scholar] [CrossRef]
- Xiang, W.; Yang, C.-Y.; Bai, L. MCL-1 Inhibition in Cancer Treatment. Onco Targets Ther. 2018, 11, 7301–7314. [Google Scholar] [CrossRef] [PubMed]
- Tron, A.E.; Belmonte, M.A.; Adam, A.; Aquila, B.M.; Boise, L.H.; Chiarparin, E.; Cidado, J.; Embrey, K.J.; Gangl, E.; Gibbons, F.D.; et al. Discovery of Mcl-1-Specific Inhibitor AZD5991 and Preclinical Activity in Multiple Myeloma and Acute Myeloid Leukemia. Nat. Commun. 2018, 9, 5341. [Google Scholar] [CrossRef] [PubMed]
- Caenepeel, S.; Brown, S.P.; Belmontes, B.; Moody, G.; Keegan, K.S.; Chui, D.; Whittington, D.A.; Huang, X.; Poppe, L.; Cheng, A.C.; et al. AMG 176, a Selective MCL1 Inhibitor, Is Effective in Hematologic Cancer Models Alone and in Combination with Established Therapies. Cancer Discov. 2018, 8, 1582–1597. [Google Scholar] [CrossRef] [PubMed]
- Oncology Pipeline. Amgen Inc. A Robust Pipeline Leveraging State-of-the-Art Science and Molecular Engineering Focused on the Pursuit of Transformative Medicines with Large Effects in Serious Diseases. Human Genetic Validation is Used to Strengthen the Evidence Base of as Many of Our Programs as Possible. Available online: https://www.amgenpipeline.com/pipeline/#oncology (accessed on 12 November 2023).
- Han, L.; Zhang, Q.; Dail, M.; Shi, C.; Cavazos, A.; Ruvolo, V.R.; Zhao, Y.; Kim, E.; Rahmani, M.; Mak, D.H.; et al. Concomitant Targeting of BCL2 with Venetoclax and MAPK Signaling with Cobimetinib in Acute Myeloid Leukemia Models. Haematologica 2020, 105, 697–707. [Google Scholar] [CrossRef] [PubMed]
- Zeidner, J.F.; Karp, J.E. Clinical Activity of Alvocidib (Flavopiridol) in Acute Myeloid Leukemia. Leuk. Res. 2015, 39, 1312–1318. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Nakauchi, Y.; Köhnke, T.; Stafford, M.; Bottomly, D.; Thomas, R.; Wilmot, B.; McWeeney, S.K.; Majeti, R.; Tyner, J.W. Integrated Analysis of Patient Samples Identifies Biomarkers for Venetoclax Efficacy and Combination Strategies in Acute Myeloid Leukemia. Nat. Cancer 2020, 1, 826–839. [Google Scholar] [CrossRef] [PubMed]
- Blombery, P.; Birkinshaw, R.W.; Nguyen, T.; Gong, J.-N.; Thompson, E.R.; Xu, Z.; Westerman, D.A.; Czabotar, P.E.; Dickinson, M.; Huang, D.C.S.; et al. Characterization of a Novel Venetoclax Resistance Mutation (BCL2 Phe104Ile) Observed in Follicular Lymphoma. Br. J. Haematol. 2019, 186, e188–e191. [Google Scholar] [CrossRef] [PubMed]
- Blombery, P.; Anderson, M.A.; Gong, J.-N.; Thijssen, R.; Birkinshaw, R.W.; Thompson, E.R.; Teh, C.E.; Nguyen, T.; Xu, Z.; Flensburg, C.; et al. Acquisition of the Recurrent Gly101Val Mutation in BCL2 Confers Resistance to Venetoclax in Patients with Progressive Chronic Lymphocytic Leukemia. Cancer Discov. 2019, 9, 342–353. [Google Scholar] [CrossRef]
- Tausch, E.; Close, W.; Dolnik, A.; Bloehdorn, J.; Chyla, B.; Bullinger, L.; Döhner, H.; Mertens, D.; Stilgenbauer, S. Venetoclax Resistance and Acquired BCL2 Mutations in Chronic Lymphocytic Leukemia. Haematologica 2019, 104, e434–e437. [Google Scholar] [CrossRef]
- Birkinshaw, R.W.; Gong, J.-N.; Luo, C.S.; Lio, D.; White, C.A.; Anderson, M.A.; Blombery, P.; Lessene, G.; Majewski, I.J.; Thijssen, R.; et al. Structures of BCL-2 in Complex with Venetoclax Reveal the Molecular Basis of Resistance Mutations. Nat. Commun. 2019, 10, 2385. [Google Scholar] [CrossRef]
- Thangavadivel, S.; Byrd, J.C. Gly101Val BCL2 Mutation: One Step Closer to Understanding Venetoclax Resistance in CLL. Cancer Discov. 2019, 9, 320–322. [Google Scholar] [CrossRef]
- Blombery, P.; Thompson, E.R.; Nguyen, T.; Birkinshaw, R.W.; Gong, J.-N.; Chen, X.; McBean, M.; Thijssen, R.; Conway, T.; Anderson, M.A.; et al. Multiple BCL2 Mutations Cooccurring with Gly101Val Emerge in Chronic Lymphocytic Leukemia Progression on Venetoclax. Blood 2020, 135, 773–777. [Google Scholar] [CrossRef] [PubMed]
- Fresquet, V.; Rieger, M.; Carolis, C.; García-Barchino, M.J.; Martinez-Climent, J.A. Acquired Mutations in BCL2 Family Proteins Conferring Resistance to the BH3 Mimetic ABT-199 in Lymphoma. Blood 2014, 123, 4111–4119. [Google Scholar] [CrossRef]
- Moujalled, D.M.; Brown, F.C.; Chua, C.C.; Dengler, M.A.; Pomilio, G.; Anstee, N.S.; Litalien, V.; Thompson, E.; Morley, T.; MacRaild, S.; et al. Acquired Mutations in BAX Confer Resistance to BH3-Mimetic Therapy in Acute Myeloid Leukemia. Blood 2023, 141, 634–644. [Google Scholar] [CrossRef] [PubMed]
- Nechiporuk, T.; Kurtz, S.E.; Nikolova, O.; Liu, T.; Jones, C.L.; D’Alessandro, A.; Culp-Hill, R.; d’Almeida, A.; Joshi, S.K.; Rosenberg, M.; et al. The TP53 Apoptotic Network Is a Primary Mediator of Resistance to BCL2 Inhibition in AML Cells. Cancer Discov. 2019, 9, 910–925. [Google Scholar] [CrossRef]
- Rahmani, M.; Nkwocha, J.; Hawkins, E.; Pei, X.; Parker, R.E.; Kmieciak, M.; Leverson, J.D.; Sampath, D.; Ferreira-Gonzalez, A.; Grant, S. Cotargeting BCL-2 and PI3K Induces BAX-Dependent Mitochondrial Apoptosis in AML Cells. Cancer Res. 2018, 78, 3075–3086. [Google Scholar] [CrossRef] [PubMed]
- Wolter, K.G.; Hsu, Y.T.; Smith, C.L.; Nechushtan, A.; Xi, X.G.; Youle, R.J. Movement of Bax from the Cytosol to Mitochondria during Apoptosis. J. Cell Biol. 1997, 139, 1281–1292. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Hou, Q.; Hansen, J.L.; Hsu, Y.-T. Complete Activation of Bax by a Single Site Mutation. Oncogene 2007, 26, 7092–7102. [Google Scholar] [CrossRef]
- Bojarczuk, K.; Sasi, B.K.; Gobessi, S.; Innocenti, I.; Pozzato, G.; Laurenti, L.; Efremov, D.G. BCR Signaling Inhibitors Differ in Their Ability to Overcome Mcl-1-Mediated Resistance of CLL B Cells to ABT-199. Blood 2016, 127, 3192–3201. [Google Scholar] [CrossRef]
- Konopleva, M.; Milella, M.; Ruvolo, P.; Watts, J.C.; Ricciardi, M.R.; Korchin, B.; McQueen, T.; Bornmann, W.; Tsao, T.; Bergamo, P.; et al. MEK Inhibition Enhances ABT-737-Induced Leukemia Cell Apoptosis via Prevention of ERK-Activated MCL-1 Induction and Modulation of MCL-1/BIM Complex. Leukemia 2012, 26, 778–787. [Google Scholar] [CrossRef]
- Vogler, M.; Butterworth, M.; Majid, A.; Walewska, R.J.; Sun, X.-M.; Dyer, M.J.S.; Cohen, G.M. Concurrent Up-Regulation of BCL-XL and BCL2A1 Induces Approximately 1000-Fold Resistance to ABT-737 in Chronic Lymphocytic Leukemia. Blood 2009, 113, 4403–4413. [Google Scholar] [CrossRef] [PubMed]
- Tromp, J.M.; Geest, C.R.; Breij, E.C.W.; Elias, J.A.; van Laar, J.; Luijks, D.M.; Kater, A.P.; Beaumont, T.; van Oers, M.H.J.; Eldering, E. Tipping the Noxa/Mcl-1 Balance Overcomes ABT-737 Resistance in Chronic Lymphocytic Leukemia. Clin. Cancer Res. 2012, 18, 487–498. [Google Scholar] [CrossRef]
- Jak, M.; van Bochove, G.G.W.; Reits, E.A.; Kallemeijn, W.W.; Tromp, J.M.; Umana, P.; Klein, C.; van Lier, R.A.W.; van Oers, M.H.J.; Eldering, E. CD40 Stimulation Sensitizes CLL Cells to Lysosomal Cell Death Induction by Type II Anti-CD20 mAb GA101. Blood 2011, 118, 5178–5188. [Google Scholar] [CrossRef] [PubMed]
- Thijssen, R.; Slinger, E.; Weller, K.; Geest, C.R.; Beaumont, T.; van Oers, M.H.J.; Kater, A.P.; Eldering, E. Resistance to ABT-199 Induced by Microenvironmental Signals in Chronic Lymphocytic Leukemia Can Be Counteracted by CD20 Antibodies or Kinase Inhibitors. Haematologica 2015, 100, e302–e306. [Google Scholar] [CrossRef] [PubMed]
- Hantschel, O.; Rix, U.; Schmidt, U.; Bürckstümmer, T.; Kneidinger, M.; Schütze, G.; Colinge, J.; Bennett, K.L.; Ellmeier, W.; Valent, P.; et al. The Btk Tyrosine Kinase Is a Major Target of the Bcr-Abl Inhibitor Dasatinib. Proc. Natl. Acad. Sci. USA 2007, 104, 13283–13288. [Google Scholar] [CrossRef] [PubMed]
- Kuusanmäki, H.; Leppä, A.-M.; Pölönen, P.; Kontro, M.; Dufva, O.; Deb, D.; Yadav, B.; Brück, O.; Kumar, A.; Everaus, H.; et al. Phenotype-Based Drug Screening Reveals Association between Venetoclax Response and Differentiation Stage in Acute Myeloid Leukemia. Haematologica 2020, 105, 708–720. [Google Scholar] [CrossRef] [PubMed]
- Pei, S.; Pollyea, D.A.; Gustafson, A.; Stevens, B.M.; Minhajuddin, M.; Fu, R.; Riemondy, K.A.; Gillen, A.E.; Sheridan, R.M.; Kim, J.; et al. Monocytic Subclones Confer Resistance to Venetoclax-Based Therapy in Patients with Acute Myeloid Leukemia. Cancer Discov. 2020, 10, 536–551. [Google Scholar] [CrossRef]
- Sharon, D.; Cathelin, S.; Mirali, S.; Di Trani, J.M.; Yanofsky, D.J.; Keon, K.A.; Rubinstein, J.L.; Schimmer, A.D.; Ketela, T.; Chan, S.M. Inhibition of Mitochondrial Translation Overcomes Venetoclax Resistance in AML through Activation of the Integrated Stress Response. Sci. Transl. Med. 2019, 11, eaax2863. [Google Scholar] [CrossRef]
- DiNardo, C.D.; Tiong, I.S.; Quaglieri, A.; MacRaild, S.; Loghavi, S.; Brown, F.C.; Thijssen, R.; Pomilio, G.; Ivey, A.; Salmon, J.M.; et al. Molecular Patterns of Response and Treatment Failure after Frontline Venetoclax Combinations in Older Patients with AML. Blood 2020, 135, 791–803. [Google Scholar] [CrossRef]
- Alwash, Y.; Khoury, J.D.; Tashakori, M.; Kanagal-Shamanna, R.; Daver, N.; Ravandi, F.; Kadia, T.M.; Konopleva, M.; Dinardo, C.D.; Issa, G.C.; et al. Development of TP53 Mutations over the Course of Therapy for Acute Myeloid Leukemia. Am. J. Hematol. 2021, 96, 1420–1428. [Google Scholar] [CrossRef]
- Choi, J.H.; Bogenberger, J.M.; Tibes, R. Targeting Apoptosis in Acute Myeloid Leukemia: Current Status and Future Directions of BCL-2 Inhibition with Venetoclax and Beyond. Target. Oncol. 2020, 15, 147–162. [Google Scholar] [CrossRef]
- Thijssen, R.; Diepstraten, S.T.; Moujalled, D.; Chew, E.; Flensburg, C.; Shi, M.X.; Dengler, M.A.; Litalien, V.; MacRaild, S.; Chen, M.; et al. Intact TP-53 Function Is Essential for Sustaining Durable Responses to BH3-Mimetic Drugs in Leukemias. Blood 2021, 137, 2721–2735. [Google Scholar] [CrossRef] [PubMed]
- Sallman, D.A.; Komrokji, R.S.; DeZern, A.E.; Sebert, M.; Garcia-Manero, G.; Rahmé, R.; Steensma, D.P.; Lehmann che, J.; Roboz, G.J.; Madelaine, I.; et al. Long Term Follow-up and Combined Phase 2 Results of Eprenetapopt (APR-246) and Azacitidine (AZA) in Patients with TP53 Mutant Myelodysplastic Syndromes (MDS) and Oligoblastic Acute Myeloid Leukemia (AML). Blood 2021, 138, 246. [Google Scholar] [CrossRef]
- Chen, L.; Chen, W.; Mysliwski, M.; Serio, J.; Ropa, J.; Abulwerdi, F.A.; Chan, R.J.; Patel, J.P.; Tallman, M.S.; Paietta, E.; et al. Mutated Ptpn11 Alters Leukemic Stem Cell Frequency and Reduces the Sensitivity of Acute Myeloid Leukemia Cells to Mcl1 Inhibition. Leukemia 2015, 29, 1290–1300. [Google Scholar] [CrossRef] [PubMed]
- Kasper, S.; Breitenbuecher, F.; Heidel, F.; Hoffarth, S.; Markova, B.; Schuler, M.; Fischer, T. Targeting MCL-1 Sensitizes FLT3-ITD-Positive Leukemias to Cytotoxic Therapies. Blood Cancer J. 2012, 2, e60. [Google Scholar] [CrossRef] [PubMed]
- Yoshimoto, G.; Miyamoto, T.; Jabbarzadeh-Tabrizi, S.; Iino, T.; Rocnik, J.L.; Kikushige, Y.; Mori, Y.; Shima, T.; Iwasaki, H.; Takenaka, K.; et al. FLT3-ITD up-Regulates MCL-1 to Promote Survival of Stem Cells in Acute Myeloid Leukemia via FLT3-ITD-Specific STAT5 Activation. Blood 2009, 114, 5034–5043. [Google Scholar] [CrossRef]
- Watanabe, D.; Nogami, A.; Okada, K.; Akiyama, H.; Umezawa, Y.; Miura, O. FLT3-ITD Activates RSK1 to Enhance Proliferation and Survival of AML Cells by Activating mTORC1 and eIF4B Cooperatively with PIM or PI3K and by Inhibiting Bad and BIM. Cancers 2019, 11, 1827. [Google Scholar] [CrossRef]
- Fang, D.D.; Zhu, H.; Tang, Q.; Wang, G.; Min, P.; Wang, Q.; Li, N.; Yang, D.; Zhai, Y. FLT3 Inhibition by Olverembatinib (HQP1351) Downregulates MCL-1 and Synergizes with BCL-2 Inhibitor Lisaftoclax (APG-2575) in Preclinical Models of FLT3-ITD Mutant Acute Myeloid Leukemia. Transl. Oncol. 2022, 15, 101244. [Google Scholar] [CrossRef]

| NCT | Study | Intervention/ Treatment | Phase | Condition/ Disease | Study Start | Estimated/ Actual Enrollment | Study Group |
|---|---|---|---|---|---|---|---|
| 04161885 | A Study Evaluating Safety and Efficacy of Venetoclax in Combination With Azacitidine Versus Standard of Care After Allogeneic Stem Cell Transplantation in Participants With Acute Myeloid Leukemia | VTX; AZA | III | AML | 26 February 2020 | 424 participants | 12 years and older |
| 03941964 | A Study of the Effectiveness of Venetoclax in Combination With Azacitidine or Decitabine in an Outpatient Setting in Patients With Acute Myeloid Leukemia Ineligible for Intensive Chemotherapy | VTX; AZA; DEC | III | AML | 15 August 2019 | 60 participants | 12 years and older |
| 02250937 | Venetoclax and Sequential Busulfan, Cladribine, and Fludarabine Phosphate Before Donor Stem Cell Transplant in Treating Patients With Acute Myelogenous Leukemia or Myelodysplastic Syndrome | VTX; BUS; CLAD; FLU | II | AML and myelodysplastic syndrome | 27 October 2014 | 116 participants | 2 years to 70 years |
| 04029688 | A Study Evaluating the Safety, Tolerability, Pharmacokinetics and Preliminary Activity of Idasanutlin in Combination With Either Chemotherapy or Venetoclax in the Treatment of Pediatric and Young Adult Participants With Relapsed/Refractory Acute Leukemias or Solid Tumors | VTX; CYT; FLU; TOP; IDA; CYC | I, II | AML, ALL, neuroblastoma, and solid tumors | 27 January 2020 | 183 participants | 0 years to 30 years |
| 04000698 | Personalized Targeted Preparative Regimen Before T-depleted Allogeneic HSCT in Children With Chemoresistent Acute Leukemias | Preparative chemotherapy before allogeneic HSCT | III | Refractory AML and refractory ALL | 15 October 2019 | 25 participants | 0 years to 25 years |
| 03844048 | An Extension Study of Venetoclax for Subjects Who Have Completed a Prior Venetoclax Clinical Trial | VTX | III | CLL, AML, MM, non-Hodgkin’s lymphoma, ALL, and cancer | 6 September 2019 | 550 participants | Children, adults, and older adults |
| 03826992 | Venetoclax Combined With Vyxeos for Participants With Relapsed or Refractory Acute Leukemia | VTX; VYX | I | Leukemia | 27 December 2018 | 21 participants | 1 year to 39 years |
| Age/Sex of Patients | Disease | Intervention/ Treatment | Therapy Effect | Adverse Events | References |
|---|---|---|---|---|---|
| 12 years/ Male | Relapsed pediatric mixed-phenotype acute leukemia | VTX + AZA | Unfulfillment of the second HSCT criterion; blast escalation; and death after 8 months post-relapse | Febrile neutropenia and lung aspergillosis | Gonzales et al. [53] |
| 17 months/ female | CBFA2T3/GLIS2 relapsed acute megakaryoblastic leukemia | VTX + AZA | MRD negative remission after one cycle; sustained through six cycles | Neutropenia | Mishra et al. [54] |
| 5 years/ male | NUP98-NSD1+/FLT3-ITD+ acute myeloid leukemia | VDAH; VDA | Proceeded to an allogeneic HSCT; in remission 301 days post-transplantation | No information | Wen et al. [55] |
| 3 years/ male | Refractory NUP98-NSD1 fusion acute myeloid leukemia | DCAG + VTX | Proceeded to an allogeneic HSCT; in remission 6 months post-transplantation | No information | Xu et al. [56] |
| 16 years/ male | Relapsed acute myeloid leukemia in Shwachman–Diamond syndrome arising from MDS | VTX + AZA | Partial bone marrow response; AML progression; and death from multi-organ failure | Diarrhea, peripheral edema, urticarial rash gingivostomatitis, and sepsis | Naviglio et al. [57] |
| 3 years/ male | Acute myeloid leukemia with myelodysplasia-related changes | VTX + AZA | Proceeded to an allogeneic HSCT; in remission 18 months post-transplantation | Myelosuppression | Wen et al. [58] |
| 5 years/ female | NPM1-mutated donor-derived MDS/AML in a patient with Fanconi anemia | VTX + AZA | Proceeded to an HSCT; in remission 1.5 years post-transplantation | Neutropenia, subdural hematoma, and pulmonary infection | Ma et al. [59] |
| Patient Number | Diagnosis | Age/Sex | Treatment Combined with VTX | Best Response | Adverse Events |
|---|---|---|---|---|---|
| 1 | Relapsed B-cell ALL | 20/F | VCR/PEG/DEX | CR | Paronychia, thrombocytopenia, anemia, and neutropenia |
| 2 | Relapsed B-cell ALL | 27/M | FLAG | PD | Sepsis, thrombocytopenia, anemia, and neutropenia |
| 3 | Relapsed B-cell ALL | 15/F | VCR/PEG/DEX | CR | Sepsis, thrombocytopenia, anemia, and neutropenia |
| 4 | B-cell ALL | 21/F | CVD | CRi | Febrile neutropenia and thrombocytopenia |
| 5 | B-cell ALL | 18/M | CVD | NR | Thrombocytopenia and neutropenia |
| 6 | B-cell ALL | 11/M | CVD | NR | Myelosuppression and hyperbilirubinemia |
| 7 | B-cell ALL | 20/F | HyperCVAD and RUX | NR | Thrombocytopenia |
| 8 | B-cell ALL | 6/F | CVD | NR | Thrombocytopenia, sepsis, and hyperbilirubinemia |
| 9 | T-cell LBL | 12/M | HyperCVAD and DEC | NR | Thrombocytopenia |
| 10 | T-cell LBL | 20/M | DEC | CR | Febrile neutropenia, thrombocytopenia, and coagulopathy |
| 11 | T-cell LBL | 20/M | HyperCVAD and NEL | CR | Sepsis and pancreatitis |
| 12 | T-cell LBL | 20/F | HyperCVAD, NEL, and PEG | CR | Thrombocytopenia and neutropenia |
| 13 | T-cell LBL | 21/M | HyperCVAD, NEL, and FLAG | CR | Thrombocytopenia |
| 14 | T-cell LBL | 21/F | CYT, IDA, and PEG | CR | Febrile neutropenia, sepsis, and myelosuppression |
| 15 | T-cell ALL | 21/M | NEL, ETO, CYC, and DEC | NR | Pneumonia, sepsis, thrombocytopenia, and hyperbilirubinemia |
| 16 | T-cell ALL | 19/M | HyperCVAD | CR | Thrombocytopenia, sepsis, and hyperbilirubinemia |
| 17 | T-cell ALL | 17/M | HyperCVAD | CRi | Febrile neutropenia and thrombocytopenia |
| 18 | ETP T-cell ALL | 19/M | FLAG, CYT, GEM, and MTX | CR | Thrombocytopenia and neutropenia |
| 19 | T-cell ALL | 18/M | HyperCVAD | NR | Thrombocytopenia and neutropenia |
| 20 | T-cell ALL | 21/M | HyperCVAD, NEL, and PEG | CR | Febrile neutropenia and thrombocytopenia |
| 21 | T-cell ALL | 22/M | NEL, PEG, and GEM | CR | None |
| NCT | Study | Intervention/ Treatment | Phase | Condition/ Disease | Study Start | Estimated/ Actual Enrollment | Study Group |
|---|---|---|---|---|---|---|---|
| 03236857 | A Study of the Safety and Pharmacokinetics of Venetoclax in Pediatric and Young Adult Patients With Relapsed or Refractory Malignancies | VTX; chemotherapy | I | AML, ALL, non-Hodgkin’s lymphoma, and neuroblastoma | 8 November 2017 | 143 participants | 0 years to 25 years |
| 04029688 | A Study Evaluating the Safety, Tolerability, Pharmacokinetics and Preliminary Activity of Idasanutlin in Combination With Either Chemotherapy or Venetoclax in Treatment of Pediatric and Young Adult Participants With Relapsed/Refractory Acute Leukemias or Solid Tumors | IDA; VTX; and chemotherapy | I, II | AML, ALL, neuroblastoma, and solid tumors | 27 January 2020 | 183 participants | 0 years to 30 years |
| 05386576 | Venetoclax in Combination With Asparaginase-Containing Pediatric-Inspired Chemotherapy in Adult Patients With Newly Diagnosed Acute Lymphoblastic Leukemia | VTX | I | ALL | 16 June 2022 | 12 participants | 18 years to 60 years |
| 03181126 | A Phase 1 Dose Escalation, Open-Label Study of Venetoclax in Combination With Navitoclax and Chemotherapy in Subjects With Relapsed/Refractory Acute Lymphoblastic Leukemia or Relapsed/Refractory Lymphoblastic Lymphoma | VTX; NAV; and chemotherapy | I | ALL and LL | 27 November 2017 | 69 participants | 4 years and older |
| 05660473 | Pediatric-inspired Regimen Combined With Venetoclax for Adolescent and Adult Patients With de Novo Philadelphia Chromosome-Negative Acute Lymphoblastic Leukemia | VTX; chemotherapy | II | Precursor cell lymphoblastic leukemia-lymphoma | 31 October 2022 | 100 participants | 14 years to 60 years |
| 05740449 | International Proof of Concept Therapeutic Stratification Trial of Molecular Anomalies in Relapsed or Refractory HEMatological Malignancies in Children, Subprotocol A: Decitabine/Venetoclax and Navitoclax in Pediatric Patients With Relapsed or Refractory Hematological Malignancies | DEC; VTX; and NAV | I, II | Relapsed/refractory ALL | 1 October 2023 | 26 participants | 1 year to 21 years |
| 05745714 | International Proof of Concept Therapeutic Stratification Trial of Molecular Anomalies in Relapsed or Refractory HEMatological Malignancies in Children, Subprotocol C Ruxolitinib + Venetoclax + Dexamethasone + Cyclophosphamide and Cytarabine in Pediatric Patients With Relapsed or Refractory Hematological Malignancies | RUX; VTX; DEXA; CP; and Ara C | I, II | Relapsed/refractory ALL | 1 October 2023 | 26 participants | 1 year to 21 years |
| 05751044 | International Proof of Concept Therapeutic Stratification Trial of Molecular Anomalies in Relapsed or Refractory HEMatological Malignancies in Children, Sub-protocol B Dasatinib + Venetoclax + Dexamethasone + Cyclophosphamide and Cytarabine in Pediatric Patients With Relapsed or Refractory Hematological Malignancies | DAS; VTX; DEXA; CP; and Ara C | I, II | Relapsed/refractory ALL | 1 October 2023 | 26 participants | 1 year to 21 years |
| 05157971 | Study Combining Venetoclax With a Pediatric-Inspired Regimen for Newly Diagnosed Adults With B Cell Ph-Like Acute Lymphoblastic Leukemia | VTX; Pred; and chemotherapy | I | BALL and Ph-like ALL | 17 March 2022 | Six participants | 18 years to 54 years |
| Age/Sex of Patients | Disease | Intervention/ Treatment | Therapy Effect | Adverse Events | References |
|---|---|---|---|---|---|
| 15 years/ male | Chronic myelomonocytic leukemia with germline GATA2 mutation | VTX + DEC | Proceeded to a myeloablative, haploidentical peripheral blood stem cell (PBSC) transplantation; in remission 1 year post-transplantation | Nausea, neutropenia, anemia, and thrombocytopenia | Molina et al. [102] |
| 11 years/ male | Relapsed blastic plasmacytoid dendritic cell neoplasm | CVAD + VTX | Proceeded to an allogeneic HSCT; in remission 200 days post-transplantation | Pneumonia, febrile neutropenia, and bacteremia | Abla et al. [103] |
| 16 years/ male | t(17;19) acute lymphoblastic leukemia | VTX + NAV | Proceeded to an allogeneic HSCT; septic shock at day + 10; and death by multi-organ failure | Neutropenia, thrombocytopenia, and diarrhea | Gottardi et al. [104] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leśniak, M.; Lipniarska, J.; Majka, P.; Lejman, M.; Zawitkowska, J. Recent Updates in Venetoclax Combination Therapies in Pediatric Hematological Malignancies. Int. J. Mol. Sci. 2023, 24, 16708. https://doi.org/10.3390/ijms242316708
Leśniak M, Lipniarska J, Majka P, Lejman M, Zawitkowska J. Recent Updates in Venetoclax Combination Therapies in Pediatric Hematological Malignancies. International Journal of Molecular Sciences. 2023; 24(23):16708. https://doi.org/10.3390/ijms242316708
Chicago/Turabian StyleLeśniak, Maria, Justyna Lipniarska, Patrycja Majka, Monika Lejman, and Joanna Zawitkowska. 2023. "Recent Updates in Venetoclax Combination Therapies in Pediatric Hematological Malignancies" International Journal of Molecular Sciences 24, no. 23: 16708. https://doi.org/10.3390/ijms242316708